You are in your early-to-mid forties. You are exhausted in a way that sleep does not fix. Your mood shifts without warning. You are not sleeping well, your periods have become unpredictable, and you feel, in your own words, like you are losing your mind.
Your doctor prescribed an antidepressant. Maybe you are already on the birth control pill. Nobody checked your hormones. Nobody mentioned perimenopause.
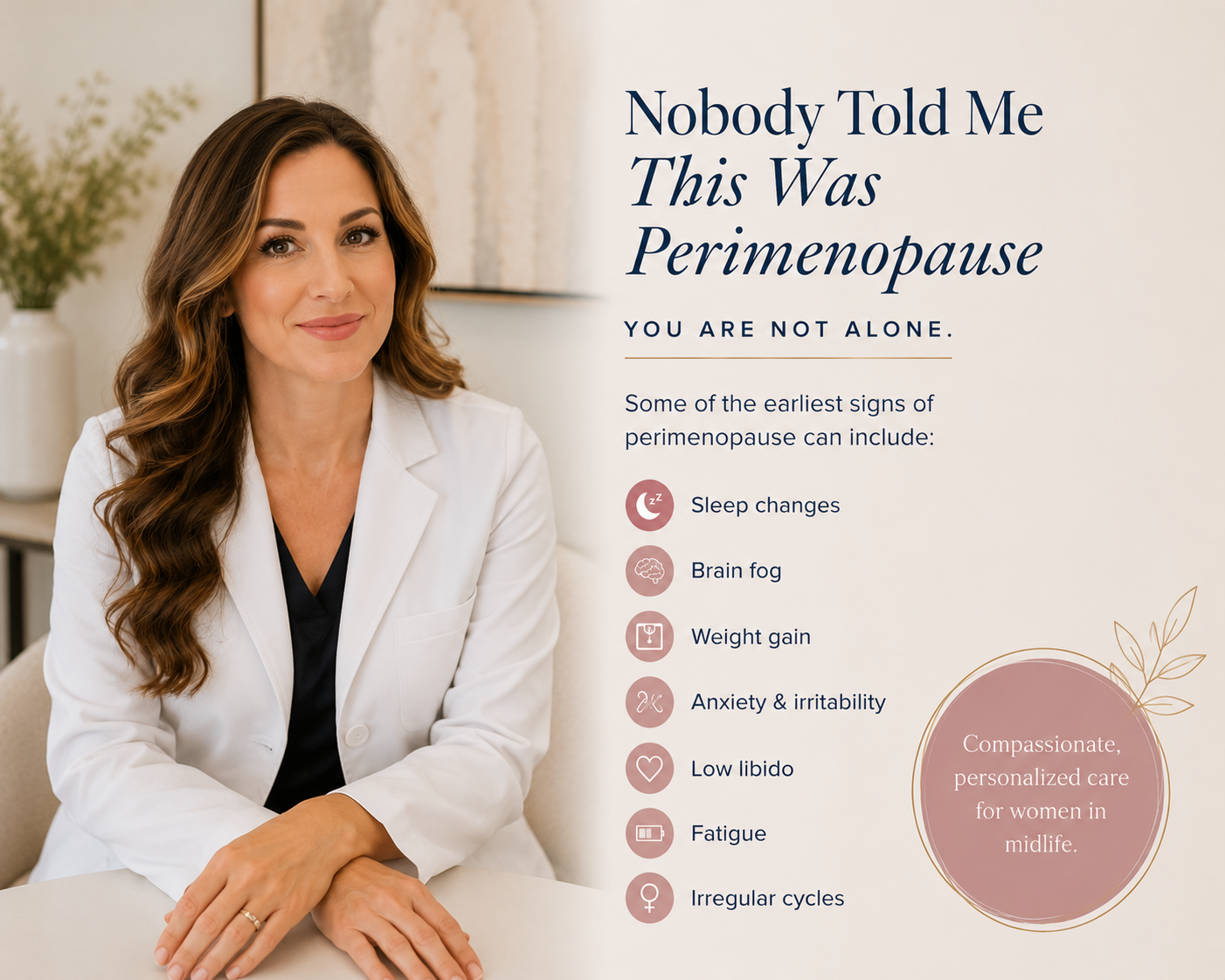
If this sounds familiar, you are not alone, and more importantly, you may not have a psychiatric disorder. You may be perimenopausal.
At Navara Health in Dallas, Texas, we specialize in hormone optimization for women navigating exactly this phase of life, and we offer telehealth appointments for patients across Texas and beyond. What we see consistently is women who have been prescribed medications for symptoms that were hormonal from the start.
What Is Perimenopause, and Why Does It Get Missed?
Perimenopause is not a brief hormonal blip before menopause arrives. It is a 4 to 8-year transition during which estradiol fluctuates significantly and progesterone progressively declines. This transition typically begins in a woman's early-to-mid 40s, sometimes earlier, and produces symptoms that look almost identical to depression and anxiety: mood instability, poor sleep, cognitive fog, fatigue, irritability, and low libido.
The overlap is not coincidental. Estrogen and progesterone have direct effects on brain chemistry. Estrogen modulates serotonin signaling, dopamine pathways, and GABA activity. When estradiol becomes erratic, so does the neurological system it regulates.
Research published in the Journal of Clinical Endocrinology and Metabolism found that it is not simply low estrogen driving perimenopausal mood symptoms. It is the variability of estradiol, combined with the loss of progesterone after ovulation, that correlates most strongly with depression and mood disruption.
This means a woman can be fully perimenopausal and still cycling, with estrogen levels that appear "normal" on a single lab draw, and while she has not yet developed hot flashes.
The risk of major depression during the menopausal transition is 2 to 4 times higher than in the premenopausal years. That is not a psychiatric statistic. That is an endocrine one.
The Problem With Prescribing an Antidepressant First
SSRIs are effective medications for true major depressive disorder. That is not disputed. But the UK's NICE guidelines specifically state that antidepressants should not be used for menopausal low mood in the absence of clinical depression, a distinction that is rarely made in primary care settings.
Beyond the question of whether SSRIs are indicated, there is a concern that almost never makes it into the prescribing conversation: SSRIs are not hormonally neutral.
Research published in Toxicology in Vitro demonstrated that all six of the most widely used SSRIs decrease androgen levels and increase the estrogen-to-androgen ratio through effects on steroidogenic enzymes. Separately, fluoxetine has been shown in animal models to disrupt the reproductive cycle and alter estrogen receptor expression. A case report in Obstetrics and Gynecology documented elevated FSH and vasomotor symptoms in a reproductive-age woman on SSRIs, a presentation indistinguishable from perimenopause.
SSRI-associated sexual dysfunction, including decreased libido, orgasmic difficulty, and reduced satisfaction, carries an odds ratio of approximately 2.3 compared to placebo and does not resolve over time the way nausea typically does. For a perimenopausal woman already experiencing declining androgens and reduced libido, this compounds the very problem the medication was prescribed to treat.
The result is a prescribing loop: hormonal changes drive mood symptoms, an SSRI is prescribed, the SSRI further disrupts androgen balance and sexual function, the woman's quality of life worsens, the dose is adjusted.
If your antidepressant is not working, or if you felt fine before your 40s and now you do not, your hormones deserve investigation before your prescription is escalated.
The Problem With Prescribing Birth Control Instead
Oral contraceptive pills are commonly prescribed to perimenopausal women for cycle regulation, heavy bleeding, and vasomotor symptoms. They do provide these benefits. But there are hormonal consequences that are rarely part of the conversation.
A systematic review and meta-analysis of 42 studies found that combined oral contraceptives decrease free testosterone by approximately 61% and increase SHBG by roughly 100 nmol/L on average. SHBG is the binding protein that renders testosterone biologically unavailable. The clinical effects of this, including reduced libido, fatigue, mood changes, and blunted motivation, are exactly the symptoms that brought many of these women to their provider in the first place.
Equally important: while a woman is on the pill, her provider cannot accurately assess her hormonal status. The HPO axis is suppressed. FSH, estradiol, and progesterone values are all altered. Perimenopause cannot be identified while a woman is on OCPs, which means the recognition of the transition, and the opportunity for early hormonal intervention, can be delayed by years.
What the Research Says About Hormonal Treatment
A landmark randomized clinical trial published in JAMA Psychiatry found that transdermal estradiol combined with intermittent micronized progesterone reduced the incidence of clinically significant depressive symptoms by nearly half (17.3% versus 32.3%) compared to placebo in euthymic perimenopausal women over 12 months. The benefit was most pronounced in early perimenopause.
A 2026 meta-analysis of 12 randomized controlled trials found that menopausal hormone therapy was associated with a statistically significant reduction in depressive symptom severity in perimenopausal women.
Hormone therapy is not a replacement for antidepressants in women with true major depressive disorder. But for women whose mood symptoms are hormonally driven, the evidence is clear that hormonal treatment should be part of the conversation, and in many cases, should come first.
What a Proper Hormone Workup Looks Like
At Navara Health, a perimenopausal evaluation is not a single FSH test. It includes a comprehensive picture of what your hormones are actually doing:
- Thyroid function (TSH, Free T4) Hypothyroidism is extremely common in women in their 40s and mimics perimenopausal symptoms almost exactly. This is always step one.
- Estradiol and progesterone Interpreted in context of cycle timing. During perimenopause, the pattern of variability is more informative than a single number.
- Total testosterone, free testosterone, and SHBG Essential for understanding libido, energy, mood, and cognitive symptoms. Critical if you are on or have recently stopped an oral contraceptive.
- DHEA-S An adrenal hormone that declines with age and contributes to energy, mood, and androgen levels independently of ovarian function.
- Fasting glucose, insulin, lipids, and HbA1c Metabolic risk shifts significantly during perimenopause and is frequently overlooked, even though it directly affects fatigue, mood, and weight.
This panel gives us an actual picture of what your hormones are doing, and it gives us the foundation to build a treatment plan that addresses the cause rather than the symptom.
Ready to get a real workup? Our clinical team in Dallas specializes in perimenopausal hormone evaluation and treatment. Telehealth appointments are available across Texas.
Book a Hormone Consultation View Our ServicesYou Deserve a Real Answer
If you are in your 40s and you do not feel like yourself, and the treatments you have been prescribed have not given you your life back, it is worth asking whether the root cause has been investigated.
Navara Health is a hormone optimization and functional wellness practice serving patients in Dallas, Texas, and via telehealth across Texas. We specialize in perimenopausal and menopausal hormone evaluation and treatment, GLP-1 and medical weight loss, and comprehensive functional lab evaluation.
The question your provider should have asked before writing that prescription is simple: could this be hormonal? If nobody has asked it yet, we will.